Patient Matching: What It Is And Why It Matters

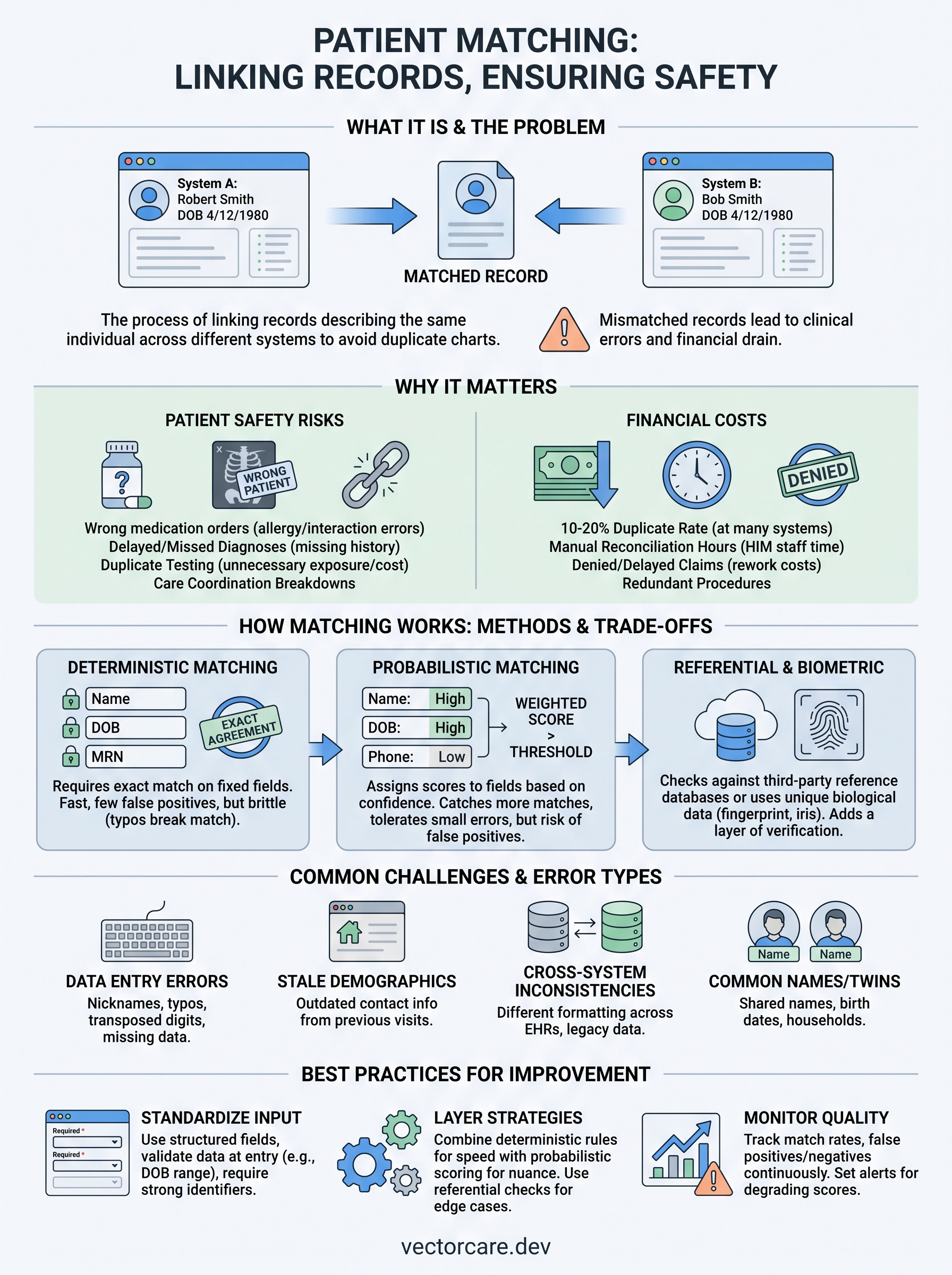
Ask two different EHR systems if "Robert Smith, DOB 4/12/1980" is the same person as "Bob Smith, DOB 4/12/1980," and you'll often get two different answers. That's the problem patient matching solves: linking records that describe the same individual across systems that store patient identity in slightly different ways. If you build software that touches clinical data, you've probably hit this wall already.
At its core, patient matching is the process of comparing demographic and clinical identifiers, name, birth date, address, insurance ID, sometimes biometric data, to determine whether two or more records belong to one patient. Health systems rely on it to avoid duplicate charts and to make sure a lab result, medication list, or referral lands on the correct patient's record instead of a stranger's.
Below, we break down how matching algorithms actually work, why deterministic and probabilistic approaches produce different results, and where the real-world matching challenges show up once you're pulling data from EPIC or other EHRs. If you're building an app that needs to integrate with clinical workflows, understanding this now saves you painful debugging later.
Why patient matching matters in healthcare
Misidentify a patient once, and you've created a problem that can follow them for years. A mismatched record means the wrong allergy list pops up during an ER visit, or a colonoscopy result gets filed under a patient who never had the procedure. Health systems don't treat patient matching as a nice-to-have data hygiene task, they treat it as a patient safety requirement, because the failure modes are severe and expensive to unwind.
Patient safety risks when matching fails
Clinicians make decisions based on what's in the chart in front of them. If that chart is missing a medication because half the patient's history lives in a duplicate record, or if it contains someone else's diagnosis because two records got merged incorrectly, the clinician is working from bad information without knowing it. The Office of the National Coordinator for Health IT has flagged patient identification errors as a persistent safety issue tied to duplicate and overlaid records, especially as data gets exchanged across more systems through initiatives like interoperability standards. The risks compound with every additional system a patient's data touches:
- Wrong-patient medication orders from incomplete allergy or drug interaction history
- Delayed diagnoses because prior imaging or lab results didn't attach to the current visit
- Duplicate testing that exposes patients to unnecessary radiation or cost
- Care coordination breakdowns when a referral or specialist note never reaches the primary chart
A single bad match doesn't just create a data problem, it creates a clinical one.
The financial cost of duplicate and mismatched records
Beyond safety, duplicate records drain money fast. Hospitals routinely spend staff hours manually reconciling charts, and every duplicate record adds administrative overhead to billing, prior authorization, and quality reporting. Denied claims tied to identity mismatches also slow down reimbursement, which matters directly to any vendor whose product depends on clean data flowing in and out of the EHR.
| Consequence of poor matching | Typical impact |
|---|---|
| Duplicate medical records | 10-20% duplicate rate reported at many large health systems |
| Denied or delayed claims | Rework costs per claim, often $25-$100+ in staff time |
| Redundant testing | Unnecessary imaging or labs repeated per encounter |
| Manual record reconciliation | Hours of HIM staff time per week at mid-size hospitals |
Why this matters if you're building on EPIC
Contracts with health systems hinge on trust, and trust starts with your app reliably identifying the right patient every single time. If you're a digital health vendor building a remote monitoring tool, a clinical decision support widget, or a referral platform, your integration has to prove it won't introduce identity errors into an already stressed system. Health system IT and compliance teams will ask pointed questions about your matching logic during vendor review, long before they ask about your UI. Getting this piece wrong doesn't just create rework, it can stall or kill a deal that took months to build. Understanding how matching actually works, which we cover next, puts you in a much stronger position to answer those questions with confidence.
How patient matching works
Matching engines compare a set of identifying attributes across two records and calculate whether they describe the same person. Every system starts with a core dataset: first and last name, date of birth, sex, address, phone number, and often a Social Security number fragment or insurance member ID. The engine scores how closely those fields align, then decides whether the records are a match, a possible match that needs human review, or clearly two different people.
Deterministic matching
Deterministic matching requires an exact agreement on a fixed set of fields, usually name, date of birth, and one more identifier like a medical record number. It's fast and produces very few false positives, but it's brittle. A typo in a middle initial, a hyphenated last name entered differently after marriage, or a transposed digit in a birth date breaks the match completely, even though it's clearly the same person. Many legacy hospital systems still lean on this method because it's simple to audit and explain to compliance teams.
Probabilistic matching
Probabilistic matching assigns weighted scores to each field based on how much it contributes to confidence in a match, then sums those scores against a threshold. Fields that rarely change, like date of birth, carry more weight than fields prone to error, like phone number. This approach catches far more true matches than deterministic logic because it tolerates small discrepancies, but it also introduces risk of false positive matches if thresholds are tuned too loosely. Most modern master patient index (MPI) tools, including those referenced in federal interoperability guidance from the ONC, use probabilistic scoring as the backbone of their identity resolution.

Deterministic matching asks for a perfect answer; probabilistic matching asks for the most likely one.
Referential and biometric matching
Newer approaches add a third layer: referential matching, which checks candidate records against a large third-party reference database of verified identities, and biometric matching, which uses fingerprints, iris scans, or facial recognition tied to a patient identifier. These methods reduce reliance on demographic data alone, which matters because demographic fields change over time, people move, change names, or share common name and birth date combinations. None of these methods work in isolation. A well-built matching pipeline layers deterministic rules for speed, probabilistic scoring for nuance, and referential checks for edge cases, which is exactly where things start to break down without careful tuning.
Common patient matching challenges and error types
Even a well-tuned matching engine runs into the same recurring problems, because the root cause isn't the algorithm, it's the data going into it. Data entry errors, inconsistent formatting, and patients who simply share common names all create noise that no scoring model fully eliminates. Knowing where these errors come from helps you design an integration that doesn't amplify them.
False positives and false negatives
Getting a match decision wrong cuts two ways, and both are dangerous in different situations. A false positive merges two different people into one record, which can mix medication histories and trigger a wrong-patient error. A false negative fails to link records that actually belong to the same person, leaving a fragmented chart with missing history. Health systems tune their thresholds constantly to balance the two, because tightening one almost always loosens the other.
Every matching system is a trade-off between merging strangers and missing the same person twice.
Data quality issues at the source
Most mismatches trace back to messy input rather than a flawed algorithm. Nicknames, maiden names, transposed digits in a birth date, and missing middle initials all reduce field-level confidence scores. Address changes are especially common since patients move far more often than their demographic fields get updated in every connected system. These are the specific error types that show up again and again:
- Name variants: "Bill" vs "William," hyphenated surnames entered inconsistently
- Transposed or truncated fields: swapped digits in date of birth or Social Security fragments
- Stale demographics: outdated address or phone number carried over from an old visit
- Twins and shared households: family members with identical addresses and similar names
- Registration shortcuts: front-desk staff entering placeholder data during high-volume intake
Cross-system inconsistencies
Fragmentation gets worse once multiple vendors and EHR instances enter the picture. A hospital's inpatient EHR, its outpatient scheduling system, and a third-party app you've built may each store the same patient under slightly different field structures. Combine that with merger-driven system consolidations, common across large health systems, and you get legacy records that were never fully reconciled. This is precisely why the Office of the National Coordinator continues to push standardized demographic data elements as a baseline for reducing cross-system identity errors, rather than leaving each vendor to interpret patient identity on its own.
Patient matching methods and technologies compared
Choosing a patient matching approach isn't a one-size-fits-all decision, it depends on your data volume, your risk tolerance, and how much control you have over the source systems feeding your app. Vendors typically pick from a handful of established matching technologies, each with different accuracy profiles and infrastructure requirements. Understanding the trade-offs before you build helps you avoid retrofitting your integration after a health system flags accuracy concerns during vendor review.
Matching engines and MPI platforms
Most large health systems run a Master Patient Index (MPI) or an enterprise-wide version, an EMPI, that centralizes identity resolution across every connected system. These platforms combine deterministic rules with probabilistic scoring, then route uncertain matches to a data steward for manual review. If you're integrating with EPIC, you're almost always matching against records that have already passed through an MPI layer, which means your app inherits whatever match quality that system produces upstream.
Your integration is only as accurate as the identity layer sitting underneath it.
Referential and biometric services
Referential matching services cross-check candidate records against a third-party database built from billions of verified consumer identities, catching matches that demographic data alone would miss. Biometric options, fingerprint or iris scanning tied to a patient ID, remove reliance on demographic fields entirely, but they require hardware and workflow changes most ambulatory settings haven't adopted yet. Both approaches add cost and complexity, so they tend to show up in large health systems or national interoperability initiatives rather than smaller vendor integrations.
| Method | How it works | Best fit |
|---|---|---|
| Deterministic rules | Exact match on fixed fields | Low-volume, high-certainty use cases |
| Probabilistic scoring | Weighted fields against a threshold | Most modern MPI/EMPI platforms |
| Referential matching | Cross-checks external identity database | Large health systems, HIE networks |
| Biometric matching | Fingerprint, iris, or facial data | High-security or high-risk settings |
Cloud-based identity resolution APIs have also entered the market, letting vendors offload matching logic instead of building scoring engines from scratch. That's a reasonable shortcut for a standalone product, but once you're pushing data into EPIC, the platform's own matching rules and your API's logic both need to agree, or you're back to reconciling duplicate records manually.
Best practices to improve match rates
You can't control every system upstream, but you can control how your own app collects, formats, and transmits patient data. Most match rate improvements come from tightening the basics: validating fields at the point of entry, standardizing formats before data ever hits an API call, and refusing to let optional fields stay blank when they're available. None of this requires exotic technology, just discipline in how your integration handles identity data at every step.
Standardize data capture at the source
Garbage in, garbage out applies directly to patient matching. If your app lets users type free-text names or addresses, you're introducing variability that no downstream algorithm can fully correct. Build structured input fields instead of open text boxes wherever possible, and normalize formatting before you send anything to the EHR. A few concrete steps make a measurable difference:
- Use dropdowns or standardized formats for state, suffix, and phone number fields instead of free text
- Capture full legal name and any known aliases or maiden names separately
- Validate date of birth against a plausible range at the point of entry, not after submission
- Require at least one strong secondary identifier, insurance member ID or medical record number, when available
- Re-verify demographics at every visit or session rather than trusting stale records
Clean data at the point of capture prevents more mismatches than any algorithm fixes downstream.
Layer multiple matching strategies
Relying on a single method almost guarantees you'll hit edge cases you didn't plan for. Combine deterministic checks for your highest-confidence fields with probabilistic scoring for everything else, and set a clear threshold for when a possible match gets routed to human review instead of auto-merged. If your volume and budget support it, add a referential matching layer for patients whose demographic data is thin or inconsistent, newborns, people experiencing homelessness, and recent immigrants are common cases where demographic-only matching fails.
Monitor match quality continuously
Matching isn't a one-time configuration, it degrades as your user base grows and as source systems change their own data. Track your false positive and false negative rates on a recurring basis, not just at launch, and set up alerts when match confidence scores start trending lower. Health system IT teams will ask about this monitoring during vendor review, so having a documented process, not just a working algorithm, strengthens your case significantly.
Patient matching in FHIR and EPIC integrations
Once you're building against EPIC, patient matching stops being an abstract concept and becomes a specific API problem you have to solve on day one. Understanding what is patient matching in a FHIR context means knowing that the standard defines a Patient resource with fields like identifier, name, birthDate, and address, but it deliberately leaves the actual matching logic up to each implementer. FHIR gives you the data model, not the algorithm, so EPIC's own identity resolution layer decides which records your app actually sees.
How FHIR structures patient identity
The HL7 FHIR Patient resource supports multiple identifier types on a single record, medical record number, insurance member ID, Social Security fragment, so a well-built app can query using more than one credential at once. That flexibility helps, but it also means poorly configured queries can pull back multiple candidate matches when your search criteria are too loose. Your app needs logic to handle a Patient.$match operation returning more than one result, rather than assuming the first record is correct.
EPIC's matching layer and what you actually control
EPIC runs its own internal matching engine ahead of anything your app touches, which means your integration inherits whatever match quality EPIC's system already produced. What you control is narrower but still critical:
| You control | EPIC controls |
|---|---|
| Query parameters sent to Patient.$match | Internal deterministic/probabilistic scoring |
| Handling multiple returned candidates | Final identity resolution within its MPI |
| Data validation before API calls | Duplicate record cleanup on its side |
Your app can't fix EPIC's identity layer, but sloppy queries can absolutely make it perform worse.
Practical steps for vendors integrating with EPIC
Submit the most specific identifiers available, don't rely on name and birth date alone when a member ID or MRN exists. Test your matching logic against edge cases before your EPIC Showroom listing goes live, since health system reviewers will ask how your app behaves when a query returns zero or multiple candidates. Getting this right the first time avoids the rework that stalls vendor onboarding for months.
Getting patient matching right going forward
Patient matching isn't a background detail you can bolt on after launch. It's the mechanism that decides whether your app builds trust with a health system or creates the exact identity errors they're already fighting to reduce. Every choice you make, from structured data capture to how you handle multiple candidates returned by a Patient.$match query, either strengthens or weakens the chart a clinician relies on.
Getting this right matters most once you're actually integrating with EPIC, where your queries interact directly with a live matching layer you don't control. Vendors who treat matching as a first-class design problem move through vendor review faster and avoid the rework that stalls contracts for months.
If you'd rather skip the months of custom FHIR development and get your matching logic right from day one, build and deploy your SMART on FHIR app with VectorCare and get it in front of health systems in weeks, not years.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.