HIPAA Consent Requirements: What Every Valid Authorization Needs

Every digital health team building a patient-facing workflow runs into the same question: does this specific data exchange need patient sign-off, and if so, what has to be on that form? Getting hipaa consent requirements wrong means rebuilding intake flows after legal review, or worse, launching something that exposes protected health information without proper authorization.
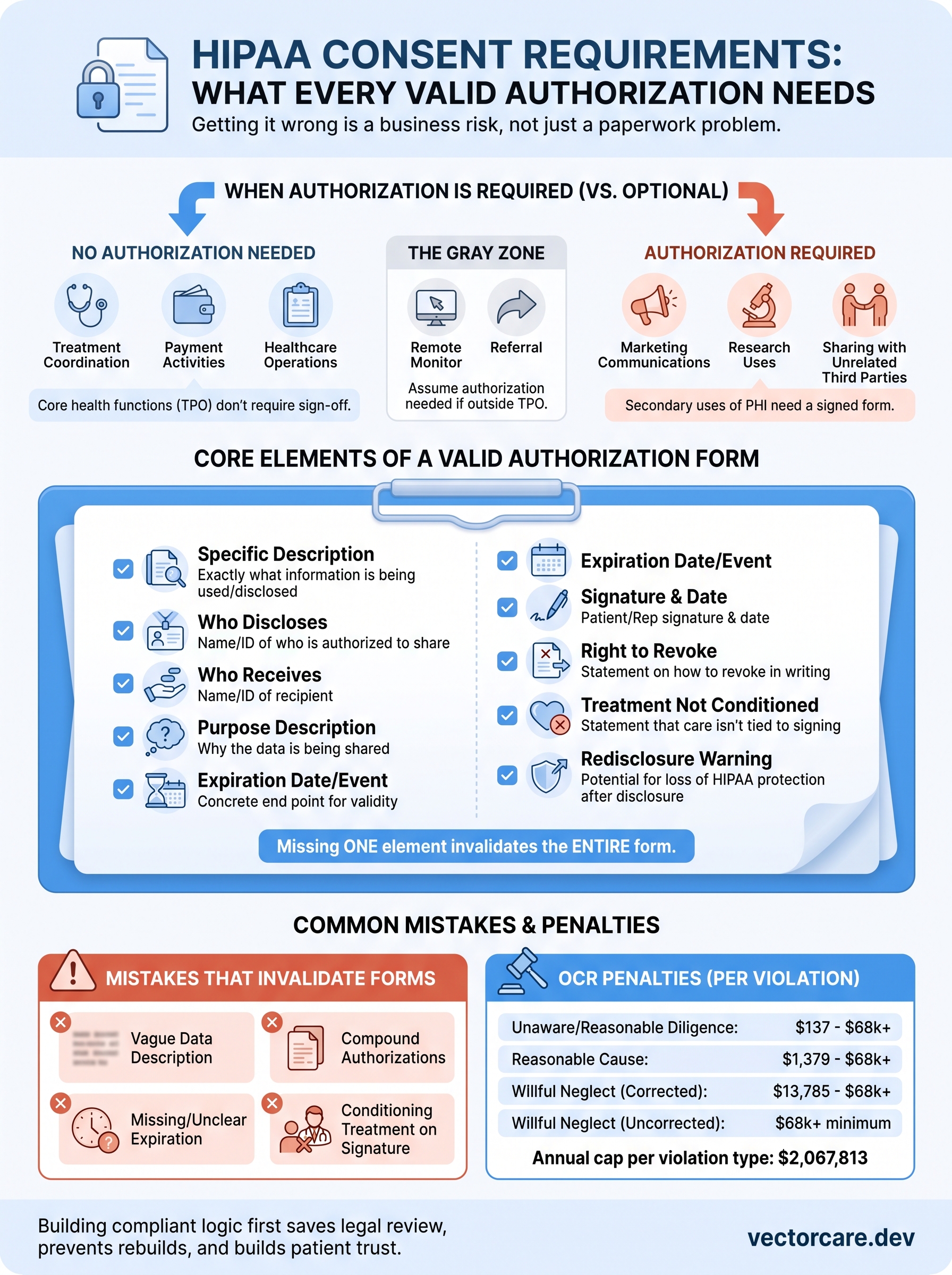
HIPAA draws a sharp line between routine uses of health information and situations that demand a signed valid authorization. Treatment, payment, and healthcare operations generally don't require patient sign-off. Marketing, research disclosures, and sharing with unrelated third parties usually do. A compliant form isn't just a signature line either; it needs specific core elements, from a description of the information involved to an expiration date and the patient's right to revoke.
This article breaks down exactly when consent is required versus optional, walks through every element a valid authorization must include, and flags the mistakes that turn a seemingly solid form into a compliance gap. If you're building a workflow that touches EPIC or any EHR, this is the groundwork you need before a single field goes live.
Why HIPAA consent requirements matter for your business
Getting hipaa consent requirements wrong isn't a paperwork problem, it's a business risk with a dollar figure attached. The Department of Health and Human Services Office for Civil Rights (OCR) enforces HIPAA through investigations that can end in corrective action plans, public settlement notices, and monetary penalties tied directly to how negligent the violation looks. A missing signature or an authorization form that never named the specific disclosure won't just get flagged in a legal review, it can become the finding that triggers a full HHS investigation into your entire platform.
What OCR penalties actually look like
OCR uses a tiered penalty structure based on the level of culpability, and the numbers escalate fast once a violation is deemed willful neglect that wasn't corrected.
| Violation Category | Penalty Per Violation | Annual Cap |
|---|---|---|
| Unaware, reasonable diligence | $137 - $68,928 | $2,067,813 |
| Reasonable cause, not willful neglect | $1,379 - $68,928 | $2,067,813 |
| Willful neglect, corrected | $13,785 - $68,928 | $2,067,813 |
| Willful neglect, not corrected | $68,928 minimum | $2,067,813 |
A single invalid authorization form can turn a routine audit into a six-figure enforcement action.
These figures come straight from the HHS civil monetary penalty schedule, and they apply per violation, not per incident. If your intake workflow pushes the same defective form to 5,000 patients, OCR can count that as 5,000 separate violations.
Why health systems scrutinize your consent flow before signing
Before any hospital lets your app touch a patient chart, someone on their compliance team is going to read your consent language line by line. Health system legal teams treat a vendor's authorization form as a proxy for how seriously that vendor takes patient data generally. If your form is missing an expiration date or doesn't spell out the right to revoke, that's often enough for a vendor risk assessment to stall, sometimes for months, while your sales team waits on a signature that never comes. EPIC's own App Orchard review process asks vendors to demonstrate exactly this kind of compliance rigor before a listing goes live, which means consent gaps show up as deployment delays long before they show up as fines.
The trust equation with patients
Patients notice sloppy consent language even when lawyers aren't in the room. Digital health products live or die on adoption, and a form that feels vague about what data gets shared with whom drives people to abandon the workflow before they finish signing up. Trust, once broken by a confusing or overreaching authorization request, is hard to rebuild inside a clinical setting where the patient already feels vulnerable. Clear consent copy that names the exact use, the exact recipient, and the exact timeframe reads as respect, not red tape, and that translates directly into completion rates for referral, intake, and remote monitoring enrollment flows.
The real cost isn't just the fine
Fines get the headlines, but the bigger cost for most digital health vendors is the rebuild. Rewriting a consent form after a health system flags it means rerouting your workflow builder, re-triggering legal review, and pushing your go-live date back weeks or months. Startups running lean engineering teams feel this hardest, because every sprint spent patching an authorization flow is a sprint not spent on the clinical feature that actually differentiates the product. Building valid authorization logic correctly the first time, before a single field goes live in EPIC, is cheaper than fixing it after a health system's compliance office sends it back.
When HIPAA authorization is required and when it isn't
Most founders assume every data exchange touching a patient chart needs a signature, but HIPAA actually carves out a wide lane where no authorization is needed at all. The Privacy Rule permits covered entities and their business associates to use and disclose protected health information for treatment, payment, and healthcare operations, often shortened to TPO, without asking the patient to sign anything. Understanding where that lane ends is the whole game when you're designing an intake or referral workflow, because building consent logic into a flow that legally doesn't need it just adds friction for zero compliance benefit.
Situations where authorization isn't required
Covered entities can share PHI freely inside the TPO exception, and a few other narrow categories the HHS Privacy Rule summary spells out directly:
- Treatment coordination: sharing labs, notes, or imaging between providers managing the same patient
- Payment activities: sending claims data to insurers or billing services
- Healthcare operations: quality assessment, care coordination, and internal audits
- Public health reporting: required disclosures to health authorities
- Court orders and law enforcement requests: disclosures compelled by valid legal process
Relying on this exception is where a lot of digital health teams get overconfident. If your app touches PHI for a purpose that isn't cleanly treatment, payment, or operations, you're outside the exception even if the use feels routine to you.
Situations where authorization is required
Anything that falls outside TPO generally needs a signed authorization, and the categories that trip up vendors most often involve secondary uses of data the patient didn't sign up for when they entered your workflow.
| Disclosure Type | Authorization Required? |
|---|---|
| Marketing communications using PHI | Yes |
| Sale of PHI to a third party | Yes |
| Research use of identifiable data | Yes |
| Psychotherapy notes shared outside treatment | Yes |
| Sharing with a non-treating third-party vendor | Yes |
| Routine care coordination between providers | No |
If the disclosure isn't treatment, payment, or operations, assume you need a signed authorization until proven otherwise.
Remote patient monitoring, referral routing, and analytics platforms sit right at this boundary, because they often pull patient data for a purpose adjacent to care but not squarely inside it. Vendors connecting patients to transportation, durable medical equipment, or home health services outside the immediate care team almost always cross into authorization territory, since that recipient isn't part of the treating relationship.
The gray zone vendors actually live in
Specific edge cases deserve their own scrutiny rather than a blanket assumption either way. Data shared with a business associate under a signed Business Associate Agreement doesn't need separate patient authorization, because the BAA already covers that relationship contractually. Disclosures for fundraising or certain limited marketing tied directly to treatment can fall under a lighter notice-and-opt-out standard rather than full authorization, which is a nuance worth confirming with counsel before you build it into a workflow. Testing this boundary early, before your workflow builder locks in field logic, saves you from retrofitting consent screens into a product that's already live inside EPIC.
How to create a valid HIPAA authorization form
Building a compliant authorization form isn't about adding a checkbox to your intake screen and calling it done. HHS spells out a specific set of core elements that every valid authorization must contain, and missing even one turns the whole document into something a covered entity can't legally rely on. Meeting hipaa consent requirements at the form level means treating each element as a required field in your workflow builder, not an optional label you can skip for a cleaner UI.
The core elements HHS requires
The HHS authorization guidance lays out exactly what a valid form must contain. Build your template around this list before you touch a single UI component:
- Specific description of the information to be used or disclosed
- Name or identification of who is authorized to make the disclosure
- Name or identification of who is authorized to receive the information
- Description of the purpose for the requested use or disclosure
- Expiration date or event that ends the authorization's validity
- Signature and date from the patient or their legal representative
- Statement of the right to revoke the authorization in writing
- Statement that treatment cannot be conditioned on signing, where applicable
- Statement of the potential for redisclosure once information leaves HIPAA's protection
Skip any one of these nine elements and the entire authorization becomes legally unusable, no matter how many signatures you collect.
Writing the required statements correctly
Statements matter as much as the fields themselves, because HHS expects specific language, not a vague gesture toward patient rights. Your revocation statement needs to tell the patient exactly how to revoke, not just that the right exists. Redisclosure language should warn the patient plainly that once their data leaves a HIPAA-covered entity, it may no longer be protected by the Privacy Rule. Vague, lawyer-proof phrasing that technically checks a box but confuses a patient reading it on a phone screen tends to fail both the compliance test and the usability test at the same time.
Building this logic into a no-code workflow
Translating these nine elements into an actual EPIC-embedded workflow means mapping each one to a distinct, required field rather than burying them in a wall of text the patient scrolls past. A well-built intake flow surfaces the purpose and recipient clearly, pulls the expiration logic from a configurable rule rather than a hardcoded date, and stores the signed record with a timestamp tied to the patient's chart. Platforms built for SMART on FHIR integration, including VectorCare's workflow builder, let you configure these fields visually so the compliance logic lives in the platform instead of scattered across custom code your engineering team has to maintain and re-audit every time a health system asks for changes.
Testing the form before it goes live
Running your draft form past legal review before deployment catches gaps a workflow builder can't catch on its own. Ask a colleague unfamiliar with the project to read the form cold and explain back what data gets shared and with whom. Confusion at that stage almost always predicts the same confusion a patient will hit during actual sign-up.
Common mistakes that invalidate HIPAA authorizations
Even teams that know the nine core elements still ship forms that fail, because the mistakes that sink an authorization are usually about how the language is written, not whether a field exists. Reviewing real OCR settlement summaries and health system compliance rejections shows the same handful of errors surfacing again and again in digital health workflows. Knowing these patterns before your workflow builder locks in a template saves you from a rebuild after a health system already flagged the form.
Vague descriptions that try to cover everything
Forms that describe the disclosed information as "health records" or "relevant data" without naming specific categories fail the specific description requirement, even if every other element is present. Compliance reviewers read this kind of language as an attempt to authorize a blank check rather than a defined disclosure. Naming the exact data type, lab results, referral notes, device readings, forces your workflow to actually think through what it's requesting instead of defaulting to broad language that feels safer but isn't.
A vague description doesn't protect you legally, it just delays the moment someone catches it.
Compound authorizations that bundle unrelated purposes
Stacking a treatment-related disclosure and a marketing use inside the same signature line is one of the fastest ways to void an authorization. HHS guidance treats compound authorizations as invalid unless the form clearly separates purposes and lets the patient opt into each independently. Bundling purposes might streamline your onboarding screen, but it creates exactly the kind of coercive signing scenario regulators are trained to flag.
Missing or unclear expiration logic
An authorization without a real expiration date, or one that lists an event so vague it can't be verified, doesn't meet the expiration date or event requirement. "Until no longer needed" isn't an expiration event a patient or auditor can check against. Tie the expiration to something concrete, a specific date, a program's end date, or a clearly defined clinical event, so the form holds up months later when someone actually needs to confirm it's still valid.
Conditioning treatment on the signature
HIPAA prohibits conditioning treatment on signing an authorization in most circumstances, and forms that blur this line by implying care won't proceed without a signature invalidate themselves outright. This mistake shows up most in referral and enrollment flows where a vendor wants the signature before granting app access, without separating the clinical service from the optional data-sharing request.
| Mistake | Why It Fails | Fix |
|---|---|---|
| Vague data description | Fails specific description requirement | Name exact data categories |
| Bundled purposes | Compound authorization, invalid under HHS rules | Separate consent per purpose |
| No real expiration event | Can't be verified or enforced | Tie to a concrete date or event |
| Treatment tied to signature | Violates conditioning prohibition | Decouple service access from consent |
Catching these patterns during a legal review, not after a health system's compliance office does, keeps your hipaa consent requirements work from turning into a rebuild cycle late in your deployment timeline.
Keeping consent compliant as you grow
A single authorization form that meets every core element today won't stay compliant forever if you're bolting on new features without revisiting the language behind them. Every new data type, recipient, or use case you add to your workflow needs the same scrutiny you gave the original form, because hipaa consent requirements apply to each disclosure, not just your first launch. Scaling into new health systems means facing new compliance reviewers, and each one will test your consent language against the same nine elements this article covered.
Building that logic once, correctly, inside a platform designed for EPIC integration saves you from re-litigating consent every time you expand. VectorCare's workflow builder handles the compliance scaffolding so your team can focus on the clinical product instead of rebuilding intake screens. Build and deploy your SMART on FHIR app in days instead of months, with consent logic baked in from the start.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.