EHR Integration: What It Is And How It Works

If you build software for healthcare and someone just asked you "do you integrate with Epic?", you already know why you're here. What is EHR integration, exactly, and why does it feel so much harder than connecting to any other API you've worked with? At its core, it's the process of connecting your application to a health system's electronic health record so patient data, orders, and workflows flow between the two systems without manual re-entry or a nurse copying values into two screens.
In practice, EHR integration today almost always means working with standards like FHIR and SMART on FHIR, the protocols that let your app securely pull and push clinical data inside platforms like Epic. It's not just a technical handshake either. It touches authentication, compliance, and clinical workflow design, which is why so many vendors underestimate the effort until they're six months into a build.
This article breaks down what EHR integration actually involves, how the data exchange works step by step, and where most vendors get stuck. If you're evaluating whether to build this yourself or find a faster path, you'll leave with a clear picture of the real requirements.
Why EHR integration matters for healthcare vendors
Health systems don't buy point solutions anymore, they buy things that live inside Epic. If your remote monitoring platform, decision support tool, or analytics dashboard requires a nurse to log into a separate portal, you've already lost the deal to a competitor who built the integration first. EHR integration is what turns your product from "another tab to open" into something that shows up inside the chart, at the point of care, where clinicians actually work. That single difference decides whether a health system signs a five-year contract or shelves your pilot after ninety days.
Contracts stall without it
Procurement teams at hospitals now ask about Epic connectivity in the first sales call, not the fifth. CIOs and clinical informatics teams have been burned too many times by tools that create extra clicks, so integration has become a gating requirement rather than a nice-to-have. Vendors who can't answer "yes, we're in the App Orchard" or "yes, we support SMART on FHIR" get filtered out before a demo is even scheduled, no matter how good the underlying product is.
A product that doesn't live inside the EHR isn't competing for the contract, it's competing to be forgotten after the pilot ends.
The real cost of building it alone
Most vendors underestimate what a custom build actually takes. Engineering teams need working knowledge of FHIR resources, OAuth 2.0 flows, and Epic's specific implementation quirks, and even experienced teams routinely spend 12 to 18 months and $250,000 or more getting from zero to a listed, production-ready app. That timeline doesn't include the ongoing maintenance burden: Epic updates its APIs, certifications need renewal, and someone has to monitor uptime for a clinical-facing system around the clock.
| Approach | Typical timeline | Typical cost | Who maintains it |
|---|---|---|---|
| Custom in-house build | 12-18 months | $250K-$500K+ | Your engineering team, indefinitely |
| Managed no-code platform | 3-6 weeks | ~$500/mo + $3K/mo per instance | The platform vendor |
Compliance isn't optional
Healthcare data carries legal weight that most SaaS integrations never touch. HIPAA and SOC2 requirements mean every data flow, storage decision, and access control has to be documented and defensible, and health systems will ask for proof before they let your app anywhere near patient records. A Business Associate Agreement isn't paperwork you file away, it's a commitment that shapes how you architect the entire integration. Vendors who treat compliance as an afterthought end up rebuilding core parts of their system once legal or the health system's security team pushes back, which is a far more expensive fix than getting it right from the start. You can read Epic's own documentation on its interoperability approach at Epic's App Orchard for a sense of the bar vendors are expected to clear before a health system will even consider a connection.
How EHR integration works in practice
Strip away the jargon and EHR integration boils down to a handshake, a request, and a response, repeated thousands of times a day across a health system. Your app asks Epic for permission, Epic verifies who's asking, and once that's settled, your app can read or write clinical data through a defined channel instead of a screen scrape or a manual export. The actual data exchange happens through an API layer that Epic exposes specifically for this purpose, and every step in that chain has to be secure, logged, and reversible if something goes wrong.
The typical flow from launch to data exchange
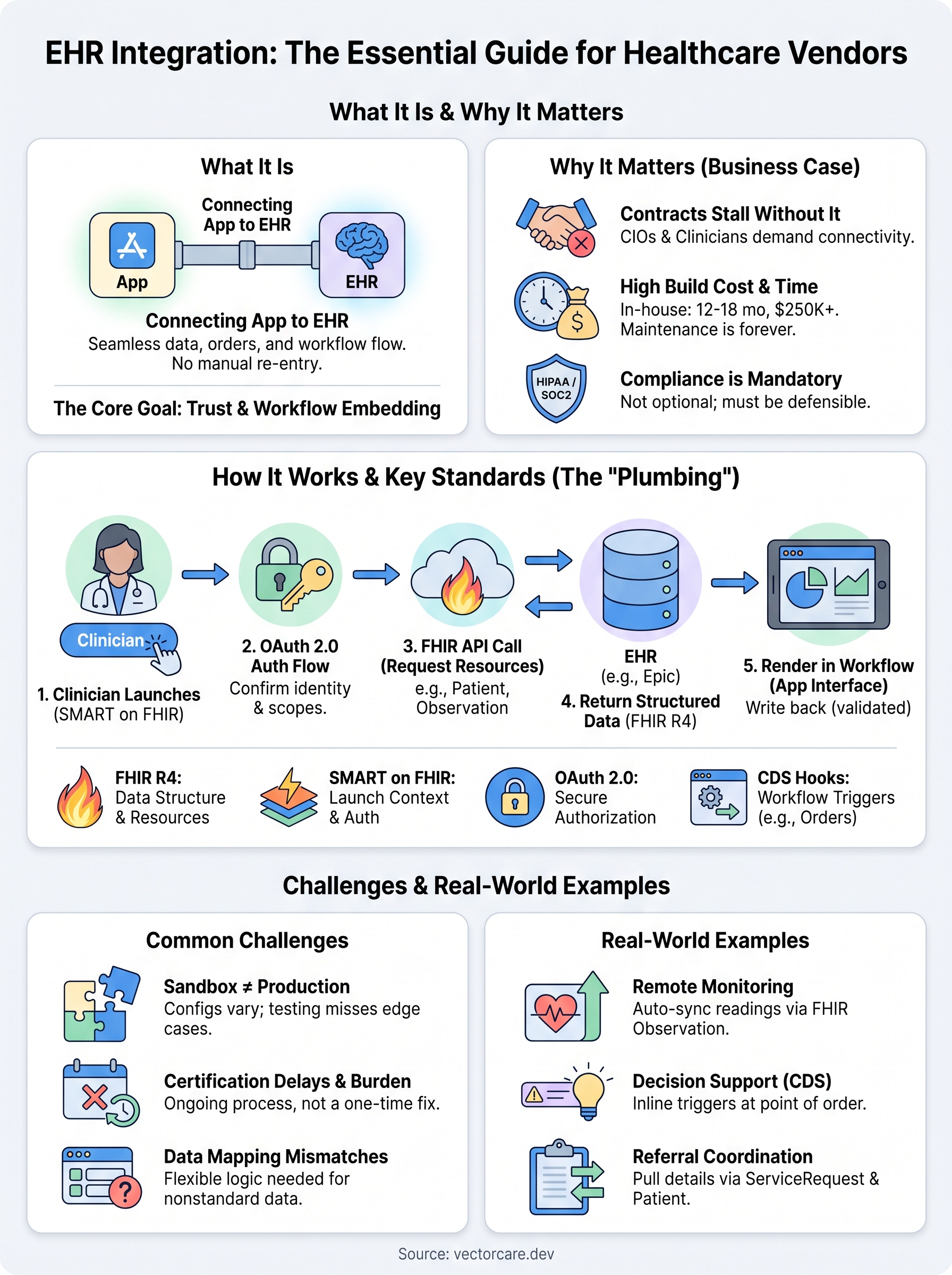
Most integrations follow a similar sequence, whether you're pulling lab results or pushing a referral order back into the chart:
- A clinician launches your app from inside Epic, either from a patient chart or a toolbar button.
- Epic redirects the launch through an OAuth 2.0 authorization flow, confirming the user's identity and the scopes your app is allowed to touch.
- Your app receives a token and uses it to call specific FHIR API endpoints, requesting only the resources it needs, like Patient, Observation, or ServiceRequest.
- Epic returns structured data in a standardized format, which your app renders inside its own interface, still embedded in the EHR session.
- If your app needs to write data back, it submits a FHIR resource through the same authenticated connection, and Epic validates it before it lands in the record.
The whole point of the exchange is that a clinician never has to leave Epic to get your app's value.
Where this plays out inside the clinical workflow
SMART on FHIR launches typically happen in one of two contexts: standalone, where your app opens independently and asks Epic for data, or EHR-launched, where a clinician clicks into your app from directly inside a patient's chart. EHR-launched integrations are what most vendors actually want, since they put your tool exactly where the clinical decision is happening, not in a separate tab the nurse has to remember to open.
Getting this sequence right the first time is harder than it looks, because every health system configures Epic slightly differently, and testing against a sandbox rarely catches every edge case you'll hit in production.
Key standards and methods behind EHR integration
Every EHR integration rests on a small set of standards, and knowing what each one actually does helps you understand why the build takes as long as it does. FHIR (Fast Healthcare Interoperability Resources) defines how clinical data gets structured into shareable resources like Patient, Observation, or MedicationRequest. SMART on FHIR builds on top of that, adding the authentication and app-launch layer that lets your product open securely inside a clinician's Epic session. Without both pieces working together, you either have data with no secure way to move it, or a secure connection with no common language to describe what's flowing through it.
The standards you'll actually work with
Most vendors end up dealing with the same handful of specs, regardless of what their app actually does clinically:
- FHIR R4: the current dominant version, defining the resource structures Epic exposes
- SMART on FHIR: governs app launch context and scoped data access
- OAuth 2.0: handles authorization, confirming who's requesting data and what they're allowed to touch
- CDS Hooks: a newer standard for triggering clinical decision support at specific points in a workflow, like ordering a medication
Get the standards right and the integration becomes a technical detail; get them wrong and it becomes the whole project.
Bulk data versus real-time calls
Not every integration needs the same method. Real-time FHIR calls make sense when a clinician needs a single patient's current data on demand, like pulling recent labs into your dashboard mid-visit. Bulk FHIR, by contrast, is built for population-level pulls, useful when your analytics or risk-scoring product needs data across thousands of patients overnight rather than one chart at a time. Choosing the wrong method here creates real problems: real-time calls at population scale will throttle against Epic's API limits, while bulk exports used for point-of-care decisions introduce lag clinicians won't tolerate.
Where certification fits in
Epic requires vendors to pass its own certification testing before an app goes live in a production environment, on top of general SMART on FHIR conformance. That process checks token handling, data validation, and error handling against Epic's specific implementation, which is exactly where many custom builds stall for weeks. The HL7 FHIR specification remains the reference point for resource definitions, and it's worth bookmarking directly rather than relying on secondhand summaries.
Common challenges in EHR integration and how to solve them
Every vendor who builds an Epic integration hits the same wall eventually, usually right after the sandbox environment lied to them. Sandbox testing rarely reflects how a real health system configures Epic, since each site customizes workflows, field mappings, and security policies differently. What passes cleanly in a test instance can throw unexpected errors in production, and debugging that gap without direct access to a hospital's Epic build is one of the most frustrating parts of the entire process.
Certification delays and maintenance burden
Getting through Epic's certification checks takes real time, and passing once doesn't mean you're done. Ongoing maintenance becomes its own job: Epic pushes API updates, security requirements shift, and your app has to keep pace or risk losing its production access entirely. Teams that treat certification as a one-time milestone instead of a recurring obligation end up scrambling every time Epic ships a new release.
Certification isn't a finish line, it's a subscription you have to keep paying into.
Data mapping and clinical context mismatches
Hospitals rarely store data the exact way your app expects it. Field-level mismatches between how a health system codes an observation and how your app parses it create silent errors that don't surface until a clinician notices something's wrong on screen. Solving this requires building flexible mapping logic rather than hardcoding assumptions about how any single Epic instance structures its data.
Practical fixes vendors rely on
Most of these problems have known workarounds, even if they take effort to implement:
- Test against multiple sandbox configurations, not just Epic's default demo environment
- Build monitoring that flags API errors in production before a clinician does
- Design mapping logic with fallback rules for missing or nonstandard fields
- Budget engineering time for recurring certification cycles, not just the initial build
Addressing these issues yourself takes sustained engineering attention, which is exactly what a managed platform absorbs on a vendor's behalf, monitoring uptime and handling recertification as Epic's requirements evolve.
Real-world examples of EHR integration
Abstract standards only make sense once you see them solving an actual clinical problem. Real-world EHR integration shows up differently depending on what a vendor's product actually does, but the underlying mechanics stay the same: pull the right FHIR resource, push it into the workflow, and keep the clinician inside Epic the whole time.
Remote patient monitoring in action
A remote patient monitoring company tracking blood pressure or glucose readings needs those values to land inside a patient's chart automatically, not sit in a separate dashboard a nurse has to check manually. Using FHIR Observation resources, the vendor's app writes readings directly into Epic on a schedule, and care teams see flagged results the moment they open the chart. That single change often cuts the time between an abnormal reading and clinical follow-up from days to hours.

Clinical decision support at the point of order
A decision support vendor building drug interaction checks or order-set recommendations relies on CDS Hooks to trigger inside Epic exactly when a physician is placing an order. Instead of a separate alert system clinicians ignore, the recommendation appears inline, tied to the specific order being written.
The best integrations disappear into the workflow so completely that clinicians forget a third-party vendor is even involved.
Referral, DME, and home health coordination
Vendors coordinating durable medical equipment or home health referrals use ServiceRequest and Patient resources to pull the referral details Epic already has, then route them to external partners without re-entering demographics or diagnosis codes by hand.
| Vendor type | Primary FHIR resource used | Workflow trigger |
|---|---|---|
| Remote patient monitoring | Observation | Scheduled device sync |
| Clinical decision support | CDS Hooks + MedicationRequest | Order entry |
| Referral/DME coordination | ServiceRequest, Patient | Referral creation |
| Healthcare analytics | Bulk FHIR | Overnight batch pull |
Each of these examples solves a different clinical problem, but every one depends on the same standards and the same certification process covered earlier.
Putting EHR integration into perspective
So what is EHR integration, really, once you strip away the acronyms? It's the plumbing that lets your app read and write patient data inside Epic without a clinician ever leaving their chart. The mechanics matter, FHIR resources, SMART on FHIR launches, OAuth tokens, CDS Hooks, but the outcome matters more: a health system trusts your product enough to let it live where care actually happens.
You now know why contracts stall without it, how the technical flow works, and where most vendors lose months to certification and maintenance they didn't budget for. That last part is the real decision point. Building it yourself costs time and engineering focus you probably need somewhere else. If you'd rather skip the 12-18 month build and get listed fast, build and deploy your SMART on FHIR app in days with VectorCare instead.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.