HIPAA Security Rule Requirements: Safeguards & Standards

If your product touches electronic protected health information (ePHI), and if you're integrating with EPIC or any other EHR system, it does, then HIPAA Security Rule requirements aren't optional reading. They're the baseline your organization must meet to operate legally and earn trust from health systems evaluating your solution.
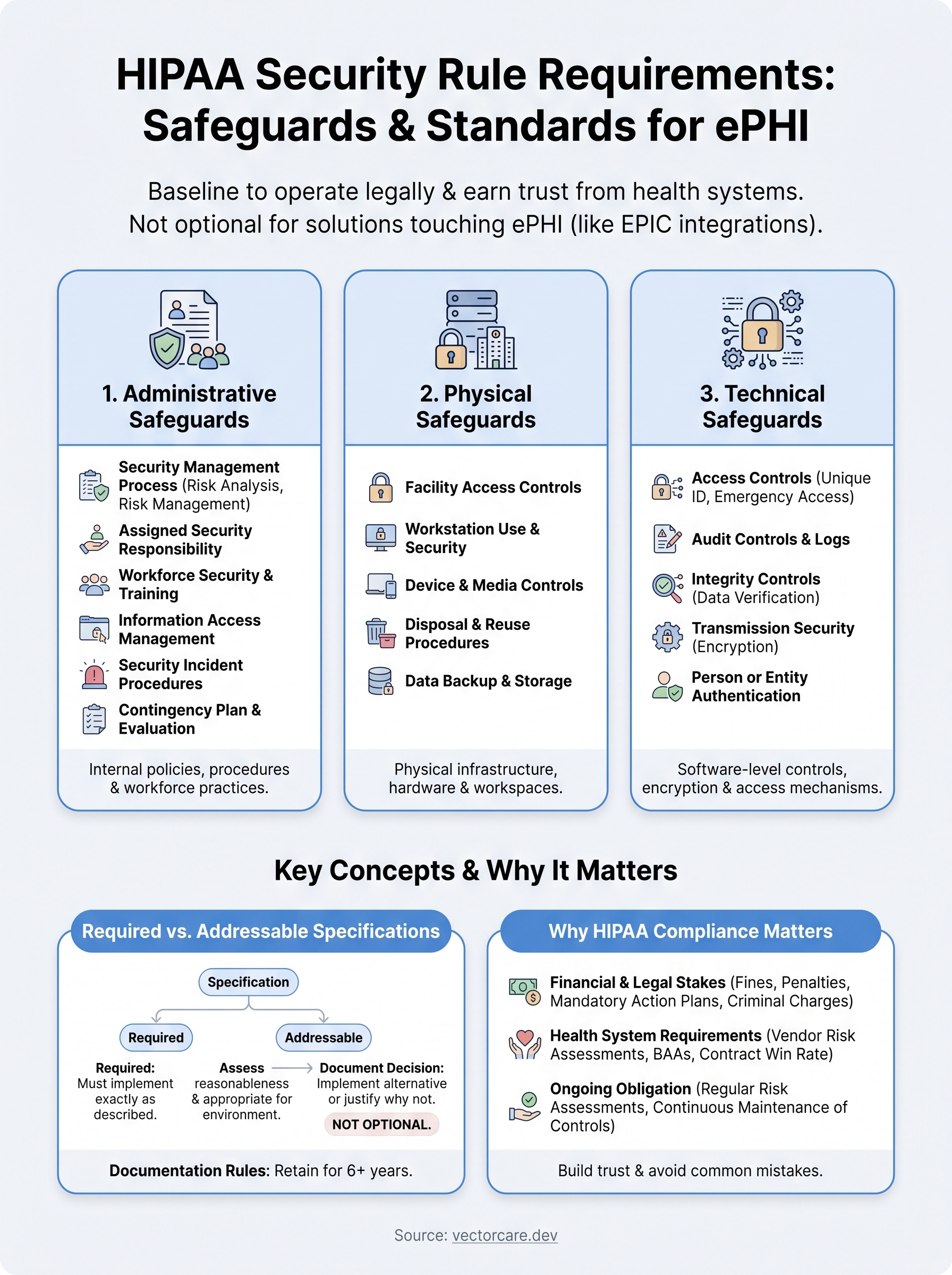
The Security Rule breaks down into three categories of safeguards: administrative, physical, and technical. Each category contains a set of standards, and each standard includes implementation specifications that are either required or addressable. That distinction matters, because "addressable" doesn't mean "optional." It means you need to assess the specification, determine whether it's reasonable and appropriate for your environment, and document your decision either way. Getting this wrong is one of the most common compliance mistakes healthcare vendors make.
This article walks through every safeguard category, standard by standard, so you understand exactly what's required and how each piece fits together. Whether you're building your compliance program from scratch or auditing an existing one, you'll leave with a clear map of what the Security Rule actually demands. At VectorCare, we build HIPAA and SOC 2 compliance directly into our no-code SMART on FHIR platform, so healthcare vendors shipping apps into EPIC don't have to solve these problems alone, but understanding the requirements yourself is still essential, and that starts here.
Why HIPAA Security Rule requirements matter
The HIPAA Security Rule has been in effect since 2005, yet enforcement actions and breach settlements continue to rise each year. Understanding why these requirements exist, and what happens when organizations fail to meet them, gives you the context you need to treat compliance as a core business function, not just a legal obligation that someone else handles.
The financial and legal stakes
The Office for Civil Rights (OCR) at the U.S. Department of Health and Human Services enforces the Security Rule, and its penalties are tiered based on the level of negligence involved. Fines range from $100 per violation at the lowest tier to $50,000 per violation at the highest, with annual caps reaching $1.9 million per violation category. A single breach involving thousands of patient records can push total penalties into the millions before you factor in legal fees, remediation costs, or mandatory audits.
Non-compliance doesn't just cost money in fines. It can trigger mandatory corrective action plans that consume significant internal resources for years after the original incident.
Beyond civil penalties, criminal charges are possible when violations involve intentional neglect or willful misuse of ePHI. Individuals, not just organizations, can face prosecution. For a healthcare vendor building a product that handles patient data, that risk extends directly to your leadership team, not just your compliance officer.
What health systems check before signing
Health systems aren't just your customers. They're also covered entities under HIPAA, which means they bear legal responsibility for the actions of every business associate they work with. When a health system evaluates your solution for EPIC integration, their security and compliance teams will ask directly whether you meet hipaa security rule requirements. If you can't demonstrate it clearly, the deal typically doesn't move forward.
Vendor risk assessments have become standard practice at most large health systems. These reviews include documentation requests, security questionnaires, and sometimes third-party audits. Your ability to provide organized evidence of your compliance posture, including policies, audit logs, incident response procedures, and technical controls, directly affects your contract win rate.
Your compliance posture also shapes the terms of your Business Associate Agreement (BAA). A health system that identifies gaps in your program will either decline to move forward or impose stricter contractual obligations with ongoing reporting requirements that slow your operations and complicate renewals.
The ongoing nature of Security Rule obligations
Most healthcare vendors underestimate how continuous Security Rule compliance actually is. It isn't a one-time certification you achieve and then file away. Risk assessments must be conducted regularly, and any meaningful change to your environment, whether that's new data flows, new infrastructure, or new third-party integrations, requires reassessment and documentation.
This ongoing burden is where many vendors run into trouble. Building and maintaining the technical controls, workforce training, and documentation the Security Rule demands requires dedicated resources that most product-focused companies haven't budgeted for.
Vendors who treat the Security Rule as foundational rather than reactive move faster in sales cycles, face fewer delays in contract negotiations, and build stronger long-term relationships with health systems. Getting compliant early and staying compliant consistently is a competitive advantage that compounds the longer you're in the market.
How to implement the HIPAA Security Rule
Implementation starts with understanding that hipaa security rule requirements aren't a checklist you complete once and forget. The rule defines what you must protect and how you must protect it, but it gives your organization flexibility in choosing specific methods based on your size, complexity, and risk profile. That flexibility is intentional, but it also means you have to make documented decisions rather than just adopt a generic template someone else built for a different environment.
Start with a formal risk analysis
The risk analysis is the foundation of your entire Security Rule program. Without a current, documented risk analysis, every other control you put in place lacks a defensible rationale. OCR has consistently cited incomplete or missing risk analyses as the leading cause of enforcement actions, which means this is not where you want to cut corners.
Your risk analysis needs to identify where ePHI exists in your environment, what threats could affect it, how likely those threats are, and what their potential impact would be.
Conduct your risk analysis before you deploy any application that handles patient data. Map every location where ePHI is created, received, maintained, or transmitted. Assign likelihood and impact scores to each identified threat, then use those scores to prioritize the controls you implement across all three safeguard categories.
Build policies before you build technical controls
Most vendors instinctively reach for technical tools first, firewalls, encryption, access controls, and then try to write policies around what they've already built. That approach creates gaps. Your policies and procedures define the expected behavior that your technical and physical controls then enforce, so writing them first gives you a coherent program rather than a collection of disconnected tools with no documented justification.
Write every policy down and tie each one to a specific Security Rule standard. Assign clear ownership so it's obvious who is responsible for maintaining each control. Set a review cadence, at minimum annually, and stick to it. When health systems request your compliance documentation during vendor assessments, an organized policy library that maps directly to the rule signals that your program is real, not assembled at the last minute.
What the HIPAA Security Rule covers
The HIPAA Security Rule applies specifically to electronic protected health information, which the rule defines as any individually identifiable health information that a covered entity or business associate creates, receives, maintains, or transmits in electronic form. That scope is narrower than HIPAA as a whole, which also covers paper records and verbal disclosures. But for healthcare vendors building software or integrating with systems like EPIC, electronic data is the primary concern, which means hipaa security rule requirements apply directly to your product.
What counts as ePHI
Any data element that connects a health condition, treatment, or payment to a specific individual qualifies as ePHI when it's stored or transmitted electronically. The rule covers 18 specific identifiers, including names, dates, geographic data, phone numbers, email addresses, Social Security numbers, and medical record numbers, among others. If your application pulls a single patient's diagnosis alongside their name from an FHIR resource, that combination is ePHI, and every system that touches it falls under Security Rule obligations.
The ePHI definition is broad enough that even a log file capturing user access to patient records can constitute ePHI if it contains identifiers tied to health information.
Your entire data pipeline matters, not just the database where records are stored. That includes API calls, message queues, temporary caches, backups, and any third-party services that receive or process patient data on your behalf.
The three safeguard categories
The Security Rule organizes all its requirements into three safeguard categories: administrative, physical, and technical. Administrative safeguards govern your internal processes, policies, and workforce practices. Physical safeguards address the physical infrastructure and hardware where ePHI is stored or processed. Technical safeguards cover the software controls, encryption, and access mechanisms that protect ePHI within your systems.

Each category contains multiple standards, and each standard includes implementation specifications. Some specifications are required, meaning you must implement them with no flexibility. Others are addressable, meaning you assess whether they're reasonable for your environment and document that decision. Together, the three categories form an integrated framework where gaps in one area undermine the protections you've built in another.
Administrative safeguards requirements
Administrative safeguards make up the largest category in the hipaa security rule requirements framework. They govern how your organization manages ePHI at a process and people level, covering your risk management program, workforce practices, incident response, and contingency planning. These aren't purely technical controls. They're the documented decisions and procedures that give every other safeguard category its direction and rationale.
Security management process
The security management process standard requires four implementation specifications: risk analysis, risk management, sanction policy, and information system activity review. Your risk analysis and risk management plan must be documented and kept current, not completed once during initial setup and then shelved. The sanction policy establishes clear consequences for workforce members who violate your security policies, and OCR expects to see those consequences applied consistently. Reviewing system activity logs on a regular schedule rounds out this standard and helps you catch unauthorized access before it escalates.

Your risk management plan should directly reference the findings from your risk analysis so auditors can trace how your controls respond to the actual threats you identified.
Assigned security responsibility and workforce management
Every organization covered by the Security Rule must designate a single individual responsible for developing and implementing security policies and procedures. That role must be assigned, documented, and active. Alongside that, workforce security requires you to define which employees need access to ePHI, implement authorization and supervision procedures, and establish a clear termination process that removes access promptly when someone leaves.
Information access management narrows this further by requiring you to restrict ePHI access to the minimum necessary for each role. Pairing that with a security awareness and training program covering malware protection, login monitoring, and password management addresses both the human and process dimensions that regulators examine first during enforcement reviews.
Security incident procedures and evaluation
Your security incident procedures must define how your team identifies, responds to, and documents security incidents involving ePHI, including incidents that don't reach the threshold of a reportable breach. The evaluation standard then requires you to periodically reassess your controls whenever your environment changes in a meaningful way. Both standards require written documentation that you can produce on request during a vendor assessment or OCR investigation.
Physical safeguards requirements
Physical safeguards address the physical infrastructure, hardware, and workspaces where ePHI is stored or accessed. Many healthcare vendors overlook this category because their products live in the cloud, but hipaa security rule requirements still apply to the physical environments your team uses, including offices, workstations, and the data centers operated by your hosting providers. If you use a managed cloud provider like AWS or Microsoft Azure, they can cover portions of the physical safeguard requirements under your Business Associate Agreement with them, but you remain responsible for documenting that coverage and filling any gaps on your end.
Assuming your cloud provider handles all physical safeguards without reviewing their scope documentation is one of the most consistent compliance gaps OCR identifies in vendor audits.
Facility access controls and workstation use
Facility access controls require you to limit physical access to your systems to authorized individuals only, while ensuring that appropriate access remains available when needed. This standard includes contingency operations procedures, a facility security plan, access control and validation procedures, and maintenance records for physical components like server rooms or locked equipment areas. Even if your team works remotely, you still need documented procedures around who can access the physical infrastructure your application runs on.
Workstation use and workstation security are separate specifications that often get merged, but each carries distinct obligations. Workstation use requires you to define the appropriate functions each workstation performs and document the physical surroundings under which those workstations operate. Workstation security then requires physical safeguards like privacy screens, locked offices, or cable locks to prevent unauthorized access to devices that store or access ePHI.
Device and media controls
Device and media controls govern how you handle the hardware and electronic media that contain ePHI throughout their lifecycle, from procurement to disposal. You need documented procedures for final disposal of ePHI, including wiping or destroying storage media before decommissioning any device. The standard also covers media re-use, accountability tracking for hardware movement, and data backup and storage when media is moved within your facility or transferred to another location.
Maintaining an inventory of devices that store or transmit ePHI gives you the visibility to apply these controls consistently and produce evidence of that control during a vendor assessment or OCR review.
Technical safeguards requirements
Technical safeguards are the software-level controls your system uses to protect ePHI from unauthorized access, modification, and transmission risks. Within the full hipaa security rule requirements framework, this category translates your documented policies into actual enforcement mechanisms built into your application, infrastructure, and data flows. Getting these controls right matters because they're the ones health system security teams verify directly during vendor assessments, often through technical questionnaires or architecture reviews.
Access controls and audit controls
Access controls require you to implement technical policies that allow only authorized users and software programs to access ePHI. This standard breaks into four specifications: unique user identification, emergency access procedures, automatic logoff, and encryption and decryption. Unique user identification means every person or system that accesses ePHI does so through an individual identifier so you can trace activity back to a specific account, not just a shared login. Emergency access procedures then ensure that authorized personnel can still reach critical data when primary systems fail, which requires a documented, tested backup path rather than an informal workaround your team improvises under pressure.

Automatic logoff is an addressable specification, but skipping it without documenting a clear rationale is a gap that OCR investigators notice quickly during audits.
Audit controls require you to implement hardware, software, or procedural mechanisms that record and examine activity in systems that contain or use ePHI. This specification is required with no flexibility, and it means your application must generate logs that capture access attempts, data retrieval events, and administrative actions. You also need a process to review those logs on a defined schedule so anomalies surface before they become incidents.
Integrity and transmission security
Integrity controls protect ePHI from improper alteration or destruction by requiring technical mechanisms to confirm that data hasn't been changed in unauthorized ways. This involves checksums, hash verification, or other validation methods applied to data at rest and in transit. Transmission security then requires you to guard against unauthorized access to ePHI moving across any electronic communications network, including your FHIR API calls between your application and EPIC. Encryption is an addressable specification under transmission security, but in practice, transmitting ePHI over unencrypted channels is indefensible given current technology, and no reasonable risk assessment supports skipping it.
Required vs addressable and documentation rules
One of the most misunderstood aspects of hipaa security rule requirements is the difference between "required" and "addressable" implementation specifications. Required specifications must be implemented exactly as the rule describes, with no substitution or exception. Addressable specifications give you flexibility, but that flexibility comes with a clear condition: you must assess each specification, decide whether it's reasonable and appropriate for your environment, and document your conclusion along with your reasoning.
What "required" and "addressable" actually mean
Addressable does not mean optional. If a specification is addressable and you determine it's reasonable and appropriate, you implement it. If you determine it isn't, you must document why and describe an equivalent alternative measure you're using instead. If neither the specification nor an alternative applies, you document that too, including your rationale. Skipping an addressable specification without any written justification is a compliance failure, and it's the kind of gap that OCR investigators identify quickly when they review your program.
The word "addressable" signals flexibility in method, not permission to ignore the underlying security objective the specification was designed to achieve.
Automatic logoff, encryption of data at rest, and audit log reviews are common examples of addressable specifications where most organizations can implement them as written. Attempting to argue that encryption is unreasonable in 2026 will not hold up under scrutiny, regardless of how the specification is labeled.
Documentation obligations
Documentation rules apply across all three safeguard categories and aren't limited to addressable specifications. Every policy, procedure, and decision your organization makes under the Security Rule must be written down and retained for at least six years from the date of creation or the date it was last in effect, whichever is later. That retention requirement applies to your risk analysis, your sanction policy, your access control procedures, your incident response records, and every other element of your compliance program.
Written documentation does two things for your organization. First, it gives your internal team a consistent reference so security practices don't depend on institutional memory that walks out the door when employees leave. Second, it gives you the evidence base you need during vendor assessments and OCR investigations. Health systems request compliance documentation as a standard part of their vendor review process, and an organized, current documentation library moves you through that process faster than any technical control alone.
Wrap-up and what to do next
Meeting hipaa security rule requirements comes down to three things: a current risk analysis, documented policies that map to each safeguard category, and technical controls your team actually maintains over time. Administrative, physical, and technical safeguards work together as a system, and a gap in any one category weakens the protections you've built in the others. Treating required and addressable specifications differently, and documenting every decision, is what separates a defensible compliance program from one that falls apart under scrutiny.
For healthcare vendors building integrations with EPIC, compliance isn't a side project. Health systems check your program before contracts move forward, and your ability to show clear evidence of your controls directly affects how fast those deals close. If you want to skip the months of engineering and compliance work that typically come with EPIC integrations, see how VectorCare handles it for you and get your application live in weeks, not quarters.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.